
Q. I would like to start fecal fat testing in my laboratory, using the Sudan black staining method. What is the best way to report fecal fat testing?
A. The gold standard of fecal fat testing is the quantitative fecal fat determination. The test was first described as a “rapid” test by the intrepid van de Kamer, et al.,1 in 1949. The method involved a 72-hour collection of feces that was then weighed, homogenized, and subjected to ether extraction. The extracted fats were quantitatively analyzed and daily output calculated. More than 6 g/day was considered pathologic, with patients with fat malabsorption usually losing more than 20 g/day. Problems included consumption of a very low-fat diet, incomplete collection, logistical problems because of voluminous output, and the general abhorrence of the method by patients and laboratory scientists in general.
Qualitative testing was first proposed by Drummey, et al.,2 in 1961, using Sudan III staining of a random specimen. The original method relied on the number and size of fat droplets to report in a graded fashion. Multiple studies have shown it to be a useful screening method for steatorrhea.3 It detects more than 90 percent of patients with clinically significant steatorrhea and is far more acceptable to patients and staff than the quantitative test. Neutral versus split fat can be reported if the sample is stained with Sudan III before and after heating and acidification.
The method used at a large reference laboratory that CAP proficiency studies use as their reporting model separates neutral and split fats utilizing heat and acidification. This is a classic method and relies on manual enumeration of fat globules on the prepared slides.4,5 A qualitative fecal fat test counts the number of fat globules in stool. This test measures two types of fat globules: neutral fat and fatty acids. Normal results are:
- Fewer than 60 neutral fat globules seen under the microscope.
- Fewer than 100 fatty acid fat globules seen under the microscope.
Two additional methods have proved useful, the acid steatocrit6 and near-infrared reflectance analysis7 (NIRA). The acid steatocrit is a gravimetric analysis of a random stool sample, with a sensitivity of 100 percent and specificity of 95 percent. The NIRA is the quantitative procedure of choice and is widely used in Europe and major U.S. reference laboratories. It is less time-consuming than the traditional 72-hour quantitative analysis and allows for measurement of fecal fat, nitrogen, and carbohydrates in a single sample.
-
-
- Van de Kamer JH, ten Bokkel Huinink H, Weyers HA. Rapid method for the determination of fat in feces. J Biol Chem. 1949;177(1):347–355.
- Drummey GD, Benson JA, Jones CM. Microscopic examination of the stool for steatorrhea. N Engl J Med. 1961;264:85–87.
- Simko V. Fecal fat microscopy. Acceptable predictive value in screening for steatorrhea. Am J Gastroenterol. 1981;75(3):204–208.
- Davidsohn I, Henry JB, eds. Clinical Diagnosis by Laboratory Methods, 14th ed. Philadelphia: W. B. Saunders; 1969:788.
- Garcia LS, ed. Clinical Microbiology Procedures Handbook, 3rd ed. Washington, DC: ASM Press; 2007:section 9.5.7.
- Amann ST, Josephson SA, Toskes PP. Acid steatocrit: a simple, rapid gravimetric method to determine steatorrhea. Am J Gastroenterol. 1997;92(12):2280–2284.
- Neumeister V, Henker J, Kaltenborn G, Sprössig C, Jaross W. Simultaneous determination of fecal fat, nitrogen, and water by near-infrared reflectance spectroscopy. J Pediatr Gastroenterol Nutr. 1997;25(4):388–393.
-
Roberta L. Zimmerman, MD
Clinical Laboratory Director
Northern Pathology Services, Grand Rapids, Minn.
Member, CAP Hematology/Clinical
Microscopy Resource Committee
Q. Who developed the formula for the corrected white blood cell count for nucleated red blood cells, and how was the formula established?
A. The formula for correcting the white blood cell count for the presence of increased circulating nucleated red blood cells (nRBCs) is a long-established maxim of hematology. Nevertheless, the origins of the formula are uncertain (to me at least), and despite my many queries to librarians, technical experts, and corporate partners, I am unable to pinpoint the exact origins of the formula. The earliest mention of the formula that I could identify in my local university library, documented without proper attribution, heralds from the 1980s,1 although I suspect the formula probably has its origins with the introduction of automated cell counters in the 1950s and 1960s.2
The formula can be derived quite easily, as outlined here.
For any given blood volume, when counting manually, the relationship between the total nucleated cell (TNC) count, the number of nRBCs (typically reported as the number of nRBCs per 100 leukocytes), and the number of leukocytes (WBC) is given by the following:
![]()
Suppose that, for a given blood sample, x µL are required to garner exactly 100 leukocytes. Thus, when factoring the volume of blood evaluated (i.e. x µL):
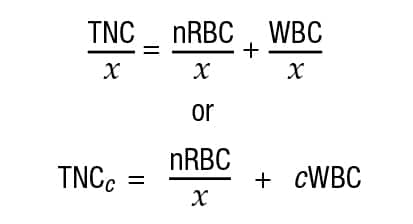
Where TNCc is the analyzer-measured WBC concentration and cWBC is the corrected WBC concentration. Thus, substituting and rearranging terms:
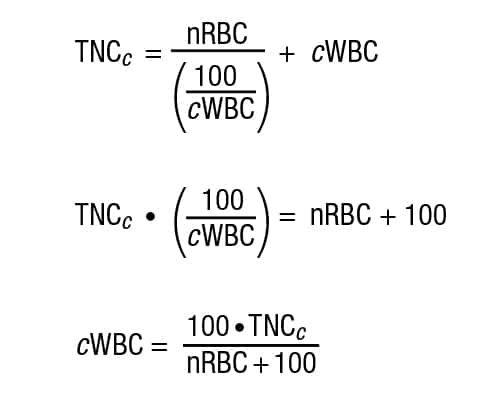
While it is certainly possible to apply the correction formula to all cases, the literature suggests that correction be invariably performed whenever nRBC is greater than five per 100 leukocytes (this assertion can also be traced back to the early 1980s,1 again without attribution). Although this cutoff is seemingly arbitrary, the logic behind it is also reasonable when the percent difference between the cWBC and TNC is considered. Above five nRBCs, the percent difference between the cWBC and TNC rises to more than 2.5 percent, which, when the two tails of a distribution are considered, would push an estimated value outside of reasonable confidence interval.
-
-
- Brown B. Hematology: Principles and Procedures, 5th ed. Philadelphia: Lea and Febiger; 1988.
- Green R, Wachsmann-Hogiu S. Development, history, and future of automated cell counters. Clin Lab Med. 2015;35(1):1–10.
-
Etienne Mahe, MD, MSc
Pathologist, Calgary Laboratory Services
Clinical Assistant Professor, Department of Pathology and Laboratory Medicine
University of Calgary, Alberta, Canada
Member, CAP Hematology/Clinical Microscopy Resource Committee